




Two journeys, one team: interdisciplinary rehabilitation in prolonged disorders of consciousness

By Lyndsey Marie, clinical lead, Askham Rehab, Cambridgeshire, UK
Abstract
Prolonged Disorders of Consciousness (PDOC) represent some of the most complex presentations within neurorehabilitation. Individuals often require long-term specialist management addressing medical stability, posture and positioning, communication, cognition, respiratory function, nutrition, psychological wellbeing, and family support. Sustained interdisciplinary collaboration is therefore essential to prevent secondary complications, optimise participation and quality of life, and—where possible—facilitate emergence and functional recovery.
This article presents two anonymised case studies from a UK specialist rehabilitation centre, illustrating differing but clinically meaningful rehabilitation trajectories within PDOC care. One case demonstrates long-term physiological stability with improved participation, therapy tolerance, and environmental engagement. The second demonstrates emergence from minimally conscious state with measurable functional progression and increased independence. Drawing on current UK evidence and national guidance, the cases demonstrate how structured interdisciplinary rehabilitation can support meaningful outcomes across the PDOC spectrum.
Background
The term Prolonged Disorder of Consciousness (PDOC) encompasses vegetative and minimally conscious states persisting beyond four weeks following severe acquired brain injury (Royal College of Physicians [RCP], 2020).
Within the UK, the clinical framework for PDOC rehabilitation is shaped primarily by the RCP National Clinical Guidelines for Prolonged Disorders of Consciousness (2020) and the British Society of Physical and Rehabilitation Medicine (BSPRM) Guidance on the Commissioning and Delivery of Services for People with PDOC in Nursing Homes (2023). Both emphasise the importance of structured interdisciplinary assessment, ongoing specialist oversight, repeated evaluation, and long-term rehabilitation management.
Recent UK evidence continues to reinforce the value of coordinated interdisciplinary rehabilitation. Turner-Stokes et al. (2022) reported that approximately 43% of individuals admitted to UK specialist rehabilitation services with PDOC demonstrated measurable emergence during rehabilitation. Siegert and Turner-Stokes (2022) further identified that variables such as physiological stability, tolerance for therapy, and ongoing interdisciplinary assessment contribute significantly to recovery trajectories.
Long-term follow-up studies additionally demonstrate that recovery trajectories in PDOC are often prolonged and non-linear. Allanson et al. (2023) followed 71 UK patients with PDOC and found that some individuals continued to demonstrate change years after injury. Wade et al. (2022) similarly highlighted the importance of balancing medical stability, specialist rehabilitation input, structured outcome measurement, and family involvement to optimise both ethical and clinical outcomes.
Importantly, meaningful outcomes in PDOC rehabilitation extend beyond emergence alone. Improvements in posture, comfort, environmental access, therapy tolerance, communication attempts, and quality of life may represent clinically significant progress even in the absence of substantial reductions in dependency scores.
Case study 1 – long-term stability, participation, and quality of life
A woman in her late thirties sustained a severe traumatic brain injury following a road traffic collision. Following prolonged acute hospital management requiring tracheostomy and PEG feeding, she was transferred to a nursing home before eventual admission to Askham Rehab for specialist rehabilitation management.
On admission, she presented with profound physical dependency, severe spasticity, limited upright tolerance, and significant postural challenges. She required 24-hour bed-based management and demonstrated inconsistent sensory responses consistent with Minimally Conscious State minus (MCS–).
Interdisciplinary rehabilitation approach
The interdisciplinary team focused on maintaining physiological stability, preventing secondary complications, and facilitating opportunities for engagement and environmental participation.
Nursing
Nursing interventions included tracheostomy management, PEG feeding, skin integrity monitoring, medication administration, respiratory care, and ongoing positioning support. These interventions were fundamental in maintaining medical stability and reducing the risk of avoidable complications.
Physiotherapy
Physiotherapy interventions focused on respiratory physiotherapy, passive mobilisation, postural management, positioning programmes, and implementation of the Symmetrikit sleep system. The aim was to optimise respiratory health, reduce spasticity, improve alignment, and increase tolerance for upright positioning.
Occupational therapy
Occupational Therapy provided specialist wheelchair seating assessments, splinting, positioning equipment, and alternative seating systems including a Kirton chair and Peapod. These interventions supported safe sitting tolerance, pressure management, comfort, and increased environmental access.
Speech and language therapy
Speech and Language Therapy implemented graded sensory stimulation programmes including music, tactile input, familiar voices, environmental modification, and structured observation of responses. Interventions additionally focused on secretion management and swallow stimulation.
Psychology and family support
Psychology supported family adjustment, emotional wellbeing, and involvement in sensory programmes. Family participation became an important component of maintaining engagement and continuity of stimulation.
Rehabilitation consultant and rehabilitation assistants
Medical oversight included spasticity management, botulinum toxin administration, goal-setting, and ongoing review of rehabilitation priorities. Rehabilitation assistants facilitated structured sensory sessions, community outings, and environmental stimulation programmes.
Progress over time
Although her Northwick Park Dependency Score (NPDS) remained relatively stable at approximately 56 between 2022 and 2025, clinically meaningful progress was observed in several important domains.
Figure 1. Northwick Park dependency score stability (2022–2025)
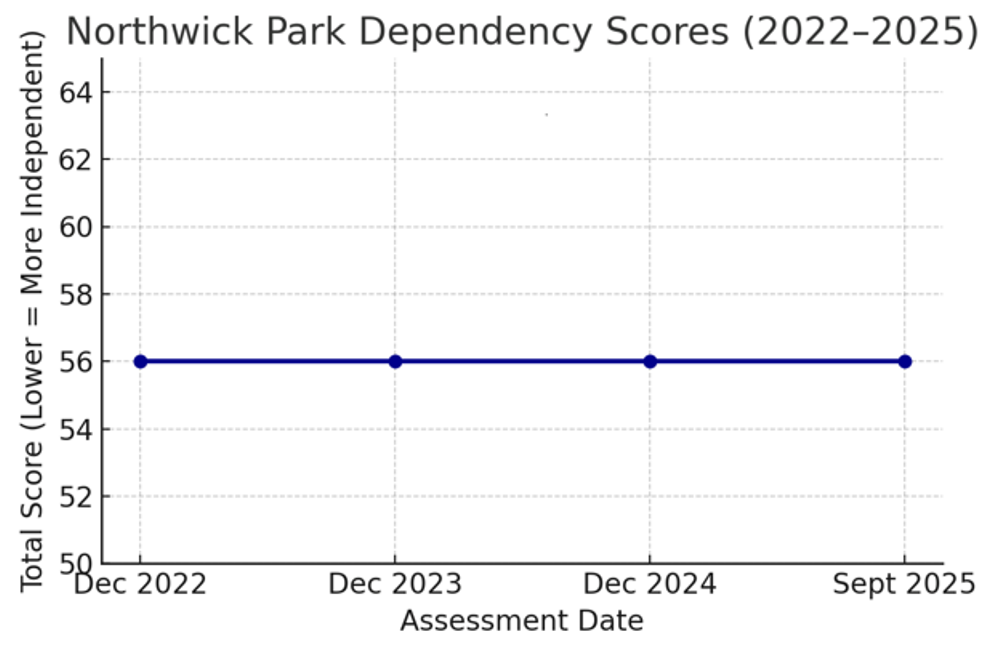
The maintenance of stable dependency scores over several years reflects successful prevention of deterioration, sustained physiological management, and effective interdisciplinary coordination.
Figure 2. Therapy tolerance progression: bed-based care to wheelchair tolerance
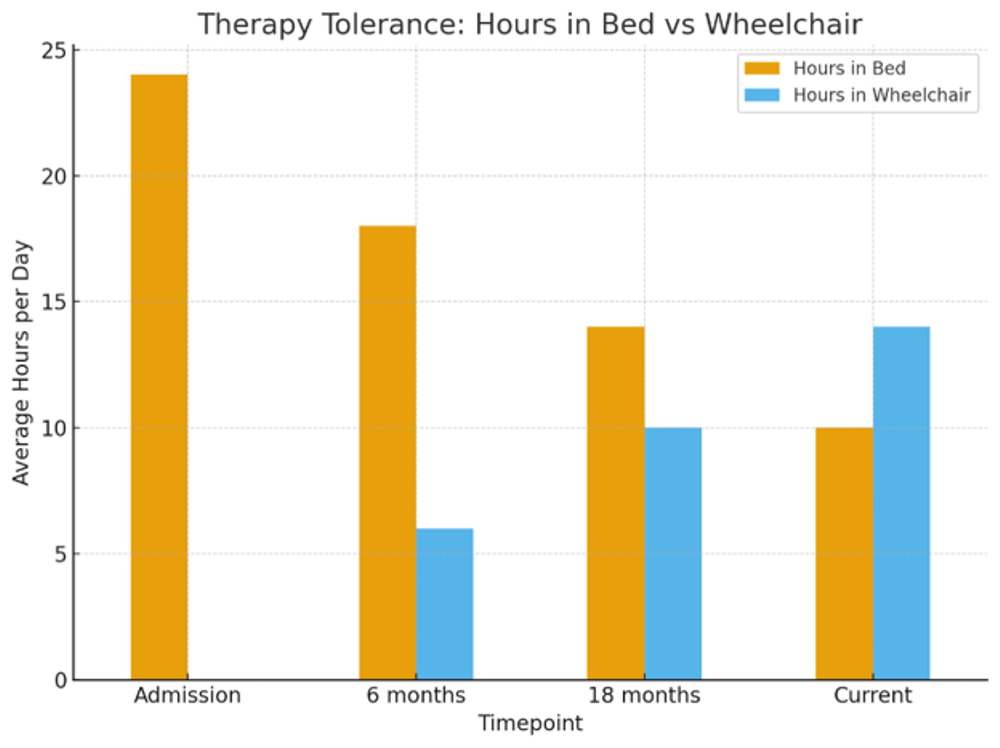
A clinically significant increase in upright tolerance was achieved over time. She progressed from requiring predominantly bed-based management to tolerating prolonged wheelchair sitting for up to eight hours daily. This enabled increased environmental access, sensory engagement, and participation in community activities.
Observable improvements included:
● Increased eye tracking and orienting to familiar voices
● Greater tolerance for sensory stimulation
● Attendance at theatre performances and concerts
● Increased time spent out of bed
● Improved postural comfort and respiratory tolerance
● Enhanced family involvement in therapy and outings
Within PDOC rehabilitation, these outcomes represent meaningful improvements in quality of life, participation, and environmental interaction despite ongoing profound dependency.
At the time of writing in 2026, her clinical stability, therapy tolerance, and interdisciplinary rehabilitation needs remain consistent, with ongoing specialist oversight and rehabilitation management.
Case study 2 – emergence and functional progression
A man in his late twenties sustained a diffuse axonal injury following a car-versus-HGV collision resulting in multiple fractures, lung contusions, a C6 fracture, and a right above-elbow amputation.
Following initial management within a Level 1 trauma centre, he was transferred to Askham Rehab approximately six to nine months post-injury. On admission, he was PEG-fed, non-verbal, bed-bound, and demonstrated minimal awareness consistent with MCS–.
Interdisciplinary rehabilitation approach
A comprehensive interdisciplinary rehabilitation programme was implemented to maximise engagement, functional progression, and independence.
Nursing
Nursing interventions focused on PEG management, medication administration, skin integrity, positioning, and ongoing medical monitoring to maintain physiological stability.
Physiotherapy
Physiotherapy interventions included postural management, strengthening programmes, respiratory rehabilitation, robotics-assisted therapy using Omego, Myro, and Pablo systems, and progression of sitting tolerance.
Occupational therapy
Occupational Therapy supported one-handed functional adaptation, executive function training, adaptive equipment provision, technology access, and activities of daily living retraining.
Speech and language therapy
Speech and Language Therapy facilitated swallow rehabilitation, communication re-establishment, and transition from PEG feeding to oral intake.
Psychology and family support
Psychology interventions focused on behavioural management, cognitive rehabilitation, emotional adjustment, and family support.
Rehabilitation assistants and medical oversight
Rehabilitation assistants supported community integration, structured therapy sessions, and participation in meaningful activities, while the Rehabilitation Consultant coordinated interdisciplinary planning and medical oversight.
Progress over time
Within six months, early signs of emergence were observed. Over time, substantial functional progression occurred across communication, nutrition, mobility, participation, and environmental interaction.
Figure 3. Therapy tolerance progression following interdisciplinary rehabilitation
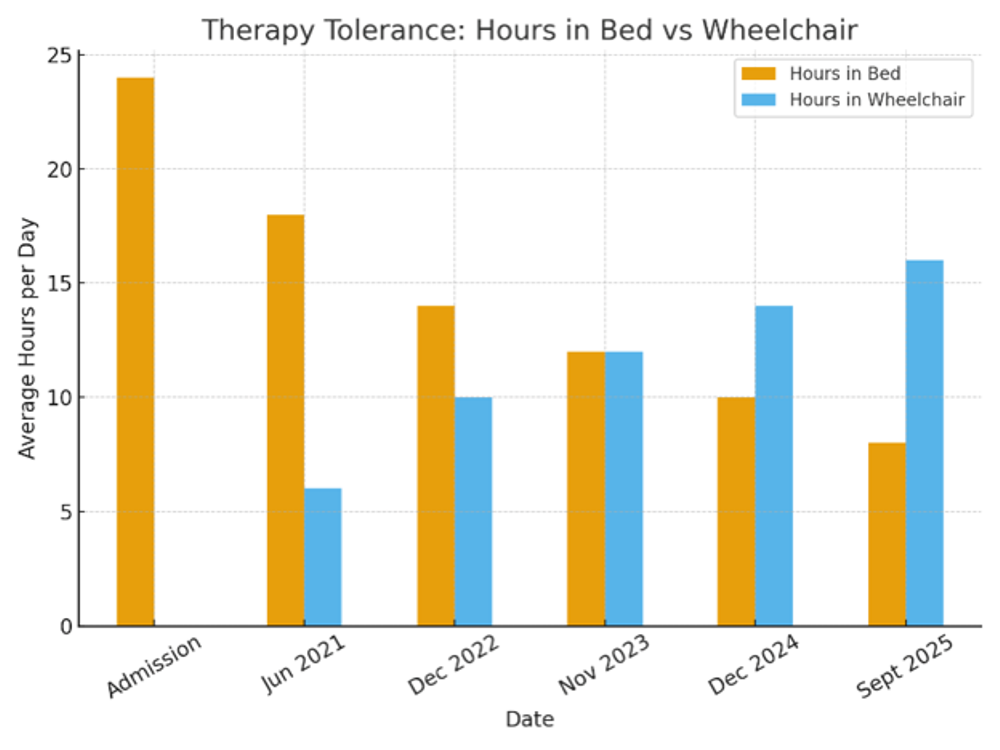
The patient progressed from requiring 24-hour bed-based management to tolerating 14–16 hours per day upright within his wheelchair, enabling sustained participation in therapies and activities.
Figure 4. Northwick Park dependency score progression following emergence
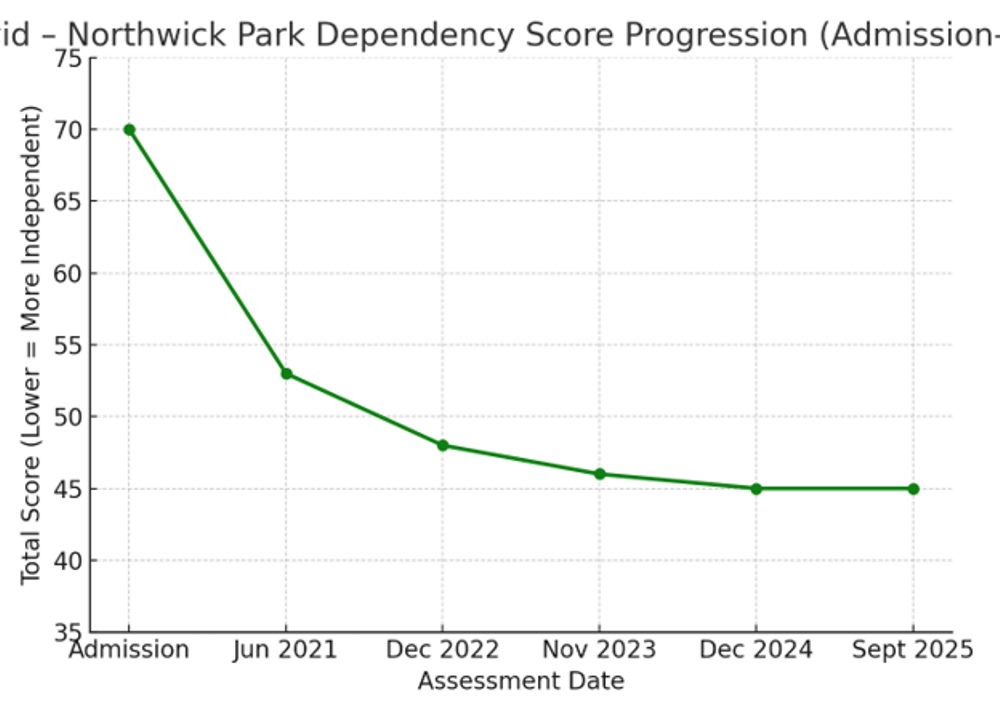
His NPDS reduced from greater than 65 on admission to the mid-40s by 2023, with stability thereafter. This reflected meaningful reductions in dependency alongside improved functional participation.
Additional outcomes included:
● Removal of PEG following successful swallow rehabilitation
● Independent oral intake (Level 7 solids, Level 0 fluids)
● Functional communication despite residual dysarthria
● Independent use of adaptive technology including tablets and TV controls
● Participation in washing and dressing tasks
● Community access including beach visits, meals out, hairdressers, and family outings
● Engagement in leisure activities including gaming, music, and television
These outcomes are consistent with UK evidence demonstrating that younger individuals with traumatic injuries receiving sustained interdisciplinary rehabilitation may demonstrate prolonged recovery trajectories and emergence from minimally conscious state.
At the time of writing in 2026, he continues to demonstrate stable functional participation and ongoing benefit from specialist interdisciplinary rehabilitation input.
Discussion
Together, these cases demonstrate differing but equally meaningful rehabilitation trajectories within PDOC care.
Case Study 1 demonstrates that meaningful rehabilitation outcomes are not limited to emergence alone. Long-term physiological stability, increased upright tolerance, environmental engagement, improved comfort, prevention of complications, and enhanced quality of life represent important and clinically significant outcomes within specialist PDOC rehabilitation.
Case Study 2 demonstrates the potential for emergence and functional progression following sustained interdisciplinary input. Improvements in dependency, communication, oral intake, mobility tolerance, and participation reflect the value of coordinated long-term rehabilitation management.
These trajectories align closely with themes identified within recent UK literature.
● Structured outcome measurement: Turner-Stokes et al. (2022) highlight the importance of tools such as NPDS and FIM+FAM in documenting subtle but meaningful progress.
● Prolonged rehabilitation trajectories: Allanson et al. (2023) demonstrate that functional change may continue years post-injury.
● Interdisciplinary governance and specialist oversight: Wade et al. (2022) emphasise the importance of coordinated interdisciplinary leadership and regular reassessment.
● Repeated multidisciplinary assessment: UK guidance highlights the risk of misdiagnosis when assessment is not undertaken collaboratively across disciplines and over time.
The cases additionally demonstrate that therapy tolerance itself may represent an important rehabilitation outcome within PDOC management. Increased upright tolerance facilitates greater environmental stimulation, respiratory optimisation, social interaction, and participation in meaningful activity, even where dependency remains high.
These cases further highlight the importance of coordinated clinical leadership in maintaining continuity across prolonged rehabilitation pathways.
By combining structured outcome measurement with flexible, person-centred rehabilitation, Askham Rehab’s approach aligns closely with both RCP (2020) and BSPRM (2023) frameworks.
Both individuals remain within ongoing specialist rehabilitation pathways at the time of writing in 2026, highlighting the long-term nature of PDOC rehabilitation management.
As illustrative case studies from a single specialist centre, these findings are not intended to be generalisable but instead highlight the diversity of meaningful rehabilitation trajectories within PDOC care. This work was previously presented in part at the PDOC Special Interest Group.
Implications for practice
● Meaningful rehabilitation outcomes in PDOC may include maintenance of physiological stability, improved therapy tolerance, enhanced comfort, environmental engagement, or emergence into functional participation.
● Long-term specialist environments remain essential for identifying subtle clinical change and preventing avoidable deterioration.
● Structured interdisciplinary goal-setting and outcome measurement support consistency and continuity of rehabilitation.
● Therapy tolerance and upright participation may represent clinically meaningful indicators of progress in PDOC rehabilitation.
● Family involvement remains central to emotional wellbeing, communication, and sustained engagement.
● Current UK evidence supports the role of sustained interdisciplinary rehabilitation in facilitating measurable benefit even years following injury.
Conclusion
Interdisciplinary rehabilitation underpins effective management across the PDOC spectrum. Whether supporting long-term stability, improving participation and quality of life, or facilitating emergence and functional progression, coordinated specialist rehabilitation enables individuals to achieve their highest possible level of health, comfort, engagement, and independence.
These cases demonstrate that meaningful progress within PDOC rehabilitation is multidimensional. While some individuals may demonstrate emergence and measurable functional recovery, others may benefit through increased participation, improved tolerance, enhanced comfort, and prevention of decline. Across all trajectories, sustained interdisciplinary collaboration remains fundamental to optimising outcomes for individuals living with PDOC.
References
Royal College of Physicians (RCP). (2020). Prolonged disorders of consciousness: national clinical guidelines. London: RCP.
British Society of Physical and Rehabilitation Medicine (BSPRM). (2023). Guidance on the Commissioning and Delivery of Services for People with Prolonged Disorders of Consciousness in Nursing Homes. London: BSPRM.
Turner-Stokes, L., Rose, H., Knight, A., Williams, H., Siegert, R., & Ashford, S. (2022). Identification using the UK FIM + FAM and cohort analysis of outcomes from a UK national clinical database. Disability and Rehabilitation, 44(12), 2763–2775.
Siegert, R. J., & Turner-Stokes, L. (2022). Prediction of emergence from prolonged disorders of consciousness: measures within the UKROC database. Clinical Rehabilitation, 37(1), 44–56.
Allanson, J., et al. (2023). How prolonged is a prolonged disorder of consciousness? Long-term follow-up of 71 consecutive admissions. Journal of Neurology, Neurosurgery & Psychiatry, 93(6), A6.
Wade, D. T., Turner-Stokes, L., Playford, E. D., Allanson, J., & Pickard, J. D. (2022). Prolonged disorders of consciousness: A response to a “critical evaluation of the new UK guidelines.” Clinical Rehabilitation, 36(9), 1049–1054.




